Difference between revisions of "Ultrasonography of renal tumors"
(Moved from Ultrasonography of the urinary system) |
m (→Evaluation: Linked) |
||
| Line 8: | Line 8: | ||
==Evaluation== | ==Evaluation== | ||
| − | A solid renal mass ([[renal tumor]]) appears in the US exam with internal echoes, without the well-defined, smooth walls seen in cysts, often with Doppler signal, and is frequently malignant or has a high malignant potential. The most common malignant renal parenchymal tumor is renal cell carcinoma (RCC), which accounts for 86% of the malignancies in the kidney. RCCs are typically isoechoic and peripherally located in the parenchyma, but can be both hypo- and hyper-echoic and are found centrally in medulla or sinus. The lesions can be multifocal and have cystic elements due to necrosis, calcifications and be multifocal (Figure 8 and Figure 9). RCC is associated with von Hippel–Lindau disease, and with tuberous sclerosis, and US has been recommended as a tool for assessment and follow-up of renal masses in these patients.<ref name="Hansen2015" /> | + | A [[solid renal mass]] ([[renal tumor]]) appears in the US exam with internal echoes, without the well-defined, smooth walls seen in cysts, often with Doppler signal, and is frequently malignant or has a high malignant potential. The most common malignant renal parenchymal tumor is renal cell carcinoma (RCC), which accounts for 86% of the malignancies in the kidney. RCCs are typically isoechoic and peripherally located in the parenchyma, but can be both hypo- and hyper-echoic and are found centrally in medulla or sinus. The lesions can be multifocal and have cystic elements due to necrosis, calcifications and be multifocal (Figure 8 and Figure 9). RCC is associated with von Hippel–Lindau disease, and with tuberous sclerosis, and US has been recommended as a tool for assessment and follow-up of renal masses in these patients.<ref name="Hansen2015" /> |
However, US is not the primary modality for the evaluation of solid tumors in the kidney, and CT is the first choice modality. Nevertheless, hemorrhagic cysts can resemble RCC on CT, but they are easily distinguished with Doppler ultrasonography. In RCCs, Doppler US often shows vessels with high velocities caused by neovascularization and arteriovenous shunting. Some RCCs are hypovascular and not distinguishable with Doppler US. Therefore, renal tumors without a Doppler signal, which are not obvious simple cysts on US and CT, should be further investigated with CEUS, as CEUS is more sensitive than both Doppler US and CT for the detection of hypovascular tumors.<ref name="Hansen2015" /> | However, US is not the primary modality for the evaluation of solid tumors in the kidney, and CT is the first choice modality. Nevertheless, hemorrhagic cysts can resemble RCC on CT, but they are easily distinguished with Doppler ultrasonography. In RCCs, Doppler US often shows vessels with high velocities caused by neovascularization and arteriovenous shunting. Some RCCs are hypovascular and not distinguishable with Doppler US. Therefore, renal tumors without a Doppler signal, which are not obvious simple cysts on US and CT, should be further investigated with CEUS, as CEUS is more sensitive than both Doppler US and CT for the detection of hypovascular tumors.<ref name="Hansen2015" /> | ||
Latest revision as of 10:55, 2 August 2019
Authors:
Mikael Häggström; Authors of Creative Commons article[1] [notes 1]
Contents
Planning
Indication for CT urography in hematuria
Most patients with macroscopic hematuria, especially when over 50 years, should undergo both cystoscopy and CT urography.[2]
Microscopic hematuria indicates further workup with cystoscopy and/or CT urography if there are significant underlying risk factors, mainly:[2]
- Male sex
- Age, especially being older than 60 years
- Smoking
- Pelvic radiation
Other indications and choices of modality
- Ultrasonography of renal tumors can generally distinguish a solid mass from a renal cyst.
- CT of renal tumors is the main method for staging a known cancer.[3]
- MRI of renal tumors is used to evaluate specific parameters thereof, such as the extent of venous involvement.[3]

Evaluation
A solid renal mass (renal tumor) appears in the US exam with internal echoes, without the well-defined, smooth walls seen in cysts, often with Doppler signal, and is frequently malignant or has a high malignant potential. The most common malignant renal parenchymal tumor is renal cell carcinoma (RCC), which accounts for 86% of the malignancies in the kidney. RCCs are typically isoechoic and peripherally located in the parenchyma, but can be both hypo- and hyper-echoic and are found centrally in medulla or sinus. The lesions can be multifocal and have cystic elements due to necrosis, calcifications and be multifocal (Figure 8 and Figure 9). RCC is associated with von Hippel–Lindau disease, and with tuberous sclerosis, and US has been recommended as a tool for assessment and follow-up of renal masses in these patients.[1]
However, US is not the primary modality for the evaluation of solid tumors in the kidney, and CT is the first choice modality. Nevertheless, hemorrhagic cysts can resemble RCC on CT, but they are easily distinguished with Doppler ultrasonography. In RCCs, Doppler US often shows vessels with high velocities caused by neovascularization and arteriovenous shunting. Some RCCs are hypovascular and not distinguishable with Doppler US. Therefore, renal tumors without a Doppler signal, which are not obvious simple cysts on US and CT, should be further investigated with CEUS, as CEUS is more sensitive than both Doppler US and CT for the detection of hypovascular tumors.[1]
Other malignant tumors in the kidney are transitional cell carcinoma and squamous cell carcinoma, which arise from the urothelium and are found the renal sinus, as well as adenocarcinoma, lymphoma and metastases, which can be found anywhere in the kidney (Figure 10).[1]
Benign solid tumors of the kidney are oncocytoma and angiomyofibroma. Oncocytoma has a varying ultrasonic appearance, but may have a central scar or calcification as a hallmark. Angiomyofibroma are often found in patients with tuberous sclerosis. They are composed of fat, smooth muscle tissue and vascular elements. The echogenicity is governed by the composition of these elements, but the lesion is often hyperechoic (Figure 11 and Figure 12).[1]
Benign tumors are difficult to separate from malignant tumors using US. Thus, solid renal masses found on US are difficult to classify and should be further evaluated with CT. In special cases of cystic or solid renal masses, additional US guided biopsy or drainage is performed to identify the histologic tumor type before a decision on surgery is made.[1]
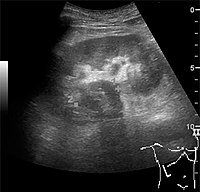
Figure 10. Solid tumor in the renal sinus seen as a hypoechoic mass, later found to be lymphoma. The ‘1’ and ‘2’ on the US image are reference points used for CT fusion (not shown).[1]

Figure 11. Angiomyolipoma seen as a hyperechoic mass in the upper pole of an adult kidney.[1]

Figure 12. Patient with tuberous sclerosis and multiple angiomyolipomas in the kidney. Measurement of kidney length on the US image is illustrated by ‘+’ and a dashed line.[1]



Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Radlines:Authorship for details.
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9 Content initially copied from: Hansen, Kristoffer; Nielsen, Michael; Ewertsen, Caroline (2015). "Ultrasonography of the Kidney: A Pictorial Review ". Diagnostics 6 (1): 2. doi:. ISSN 2075-4418. (CC-BY 4.0)
- ↑ 2.0 2.1 USA: Raman, Siva P.; Fishman, Elliot K. (2014). "Bladder Malignancies on CT: The Underrated Role of CT in Diagnosis ". American Journal of Roentgenology 203 (2): 347–354. doi:. ISSN 0361-803X.
- ↑ 3.0 3.1 Bradley, A J; Lim, Y Y (2014). "Imaging of renal masses and staging of renal tumours ". Imaging 23 (1): 20110081. doi:. ISSN 0965-6812.