CT of the abdomen and pelvis
Author:
Mikael Häggström [notes 1]
Emergencies
Locations
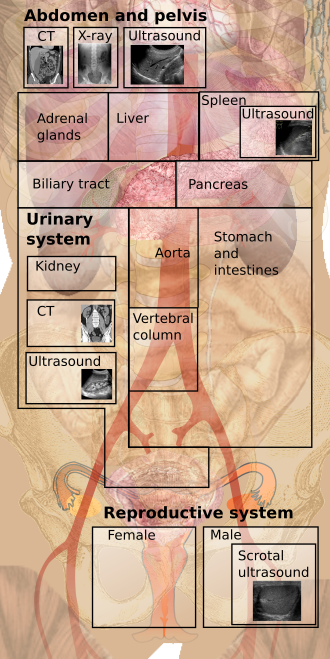

Basic screening
Compare with any previous exam.
Example approach:
Liver, spleen, adrenals and kidneys
Scan through the entire volumes and look mainly for focal changes.
- The thickness of the adrenal glands is normally up to 1.0 cm.[1]
Further information:


- Look at the gallbladder and biliary tract for visible stones or dilatation.
- Also exclude hydronephrosis of the kidneys.
Free gas
Switch to a lung window (wide attenuation range), with main focus on the anterior wall, where gas most likely appears.
While in this window, also have a glance at the bases of the lungs for pleural fluid or obvious lung tumors.
Free fluid
Look mainly in the hepatorenal recess and inferiorly in the pelvis.
Lymph nodes
Look mainly around the aorta and iliac arteries.
| Retrocrural space | 6 mm[2] |
| Paracardiac | 8 mm[2] |
| Gastrohepatic ligament | 8 mm[2] |
| Upper paraaortic region | 9 mm[2] |
| Portacaval space | 10 mm[2] |
| Porta hepatis | 7 mm[2] |
| Lower paraaortic region | 11 mm[2] |
Small intestine
On CT scans, a small intestinal diameter of over 2.5 cm is considered abnormally dilated.[3][4][5]
Large intestine

- Exclude dilatations.
- Check the intestinal wall for any thickening of over 5 mm.[7] Focal, irregular and asymmetrical gastrointestinal wall thickening suggests a malignancy.[7] Segmental or diffuse gastrointestinal wall thickening is most often due to ischemic, inflammatory or infectious disease.[7]
Aorta
- Exclude aneurysm, which is generally defined as over 3 cm.[8]
- Further information: CT of abdominal aneurysm
Urinary bladder
Quick look for obvious wall thickening.
Reproductive system
Males: Quick look at the prostate for obvious irregularities.

Prostate cancer.

Females: Look mainly at the locations of the ovaries for any expansions.
Skeleton
Any signs of damage.
Other extra-peritoneal volumes
Quick overview to exclude mainly obvious soft tissue expansions such as hematomas (see CT of muscular hematoma).
Report
Example report in a normal abdomen:
|
No free gas or ascites
|
- See also: General notes on reporting
Special cases
Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Radlines:Authorship for details.
References
- ↑ Antonio Carlos A. Westphalen and Bonnie N. Joe (2006). "CT and MRI of Adrenal Masses ". Appl Radiol 35 (8): 10–26. Archived from the original. .
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 Dorfman, R E; Alpern, M B; Gross, B H; Sandler, M A (1991). "Upper abdominal lymph nodes: criteria for normal size determined with CT. ". Radiology 180 (2): 319–322. doi:. ISSN 0033-8419.
- ↑ Ali Nawaz Khan (2016-09-22). Small-Bowel Obstruction Imaging. Medscape. Retrieved on 2017-02-07.
- ↑ . Abdominal X-ray - Abnormal bowel gas pattern. radiologymasterclass.co.uk. Retrieved on 2017-02-07.
- ↑ Gazelle, G S; Goldberg, M A; Wittenberg, J; Halpern, E F; Pinkney, L; Mueller, P R (1994). "Efficacy of CT in distinguishing small-bowel obstruction from other causes of small-bowel dilatation. ". American Journal of Roentgenology 162 (1): 43–47. doi:. ISSN 0361-803X.
- ↑ "Deficient Pms2, ERCC1, Ku86, CcOI in field defects during progression to colon cancer ". J Vis Exp (41). 2010. doi:. PMID 20689513.
- ↑ 7.0 7.1 7.2 Fernandes, Teresa; Oliveira, Maria I.; Castro, Ricardo; Araújo, Bruno; Viamonte, Bárbara; Cunha, Rui (2014). "Bowel wall thickening at CT: simplifying the diagnosis ". Insights into Imaging 5 (2): 195–208. doi:. ISSN 1869-4101.
- ↑ "ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Associations for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (writing committee to develop guidelines for the management of patients with peripheral arterial disease)—summary of recommendations ". J Vasc Interv Radiol 17 (9): 1383–97; quiz 1398. September 2006. doi:. PMID 16990459.